India’s National HPV Vaccination Drive (2026)
Strategic Public Health Reform for Cervical Cancer Elimination
Syllabus: UPSC GS II – Government Policies & Health; Social Sector Interventions)
Introduction
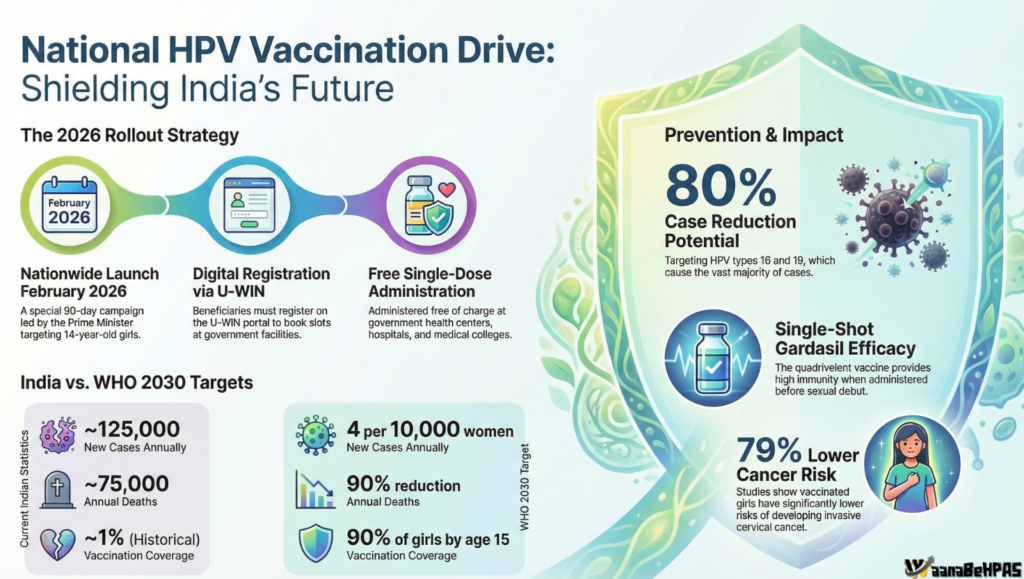
India is embarking on a transformative public health reform with the nationwide launch of the Human Papillomavirus (HPV) Vaccination Campaign on 28 February 2026 from Ajmer. The initiative represents a historic shift from fragmented, opportunistic cervical cancer screening toward primary prevention at scale.
For UPSC aspirants, this development is significant not only as a health programme but as a case study in:
- Preventive healthcare governance
- Gender-focused welfare policy
- Evidence-based decision-making
- Health systems strengthening
I. The Strategic Imperative: Why HPV Vaccination Matters
1. Disease Burden in India
Cervical cancer remains the second most common cancer among Indian women.
- India accounts for nearly one-fifth of the global cervical cancer burden
- Annual incidence: ~80,000–96,000 new cases
- Annual deaths: ~42,000–60,000
- Over 80% linked to persistent infection with high-risk HPV types 16 & 18
The socio-economic implications are severe:
- Treatment costs create a “poverty trap”
- 78% of families rely on personal savings for non-medical expenses
- High dropout rates in treatment due to financial strain
Thus, vaccination is not merely a clinical tool — it is an economic and gender equity intervention.
2. India’s Commitment to WHO 90-70-90 Targets
India aligns with the World Health Organization’s cervical cancer elimination strategy:
- 90% of girls fully vaccinated by age 15
- 70% of women screened by ages 35 & 45
- 90% of women with cervical disease treated
The 2026 drive marks the beginning of India’s elimination roadmap.
II. Clinical Amalgamation: Vaccine Portfolio & Scientific Evidence
1. Available HPV Vaccines in India
| Vaccine | Manufacturer | Strains Covered | Use Case |
|---|---|---|---|
| CERVAVAC | Serum Institute of India | 6, 11, 16, 18 | Indigenous; NTAGI recommended (awaiting WHO PQ) |
| Gardasil | Merck | 6, 11, 16, 18 | 2026 National Campaign |
| Cervarix | GSK | 16, 18 | Private market |
| Gardasil 9 | Merck | 9 HPV strains | Private market |
2. The Single-Dose Breakthrough
A landmark 10-year Indian cohort study (IARC-backed) demonstrated:
- 95.4% efficacy of single-dose vaccination against persistent HPV 16/18 infection.
Strategic importance:
- Reduces “loss to follow-up”
- Easier logistics
- Cost-effective
- Highly suitable for rural India
This evidence allows India to adopt a single-dose strategy, making large-scale immunization feasible.
III. The 2026 National Campaign: Operational Architecture
The February 2026 initiative is a special national campaign, distinct from but paving the way for integration into the Universal Immunization Programme (UIP).
Target Population
- Primary focus: 14-year-old girls
- Ensures vaccination prior to HPV exposure
1. Procurement Strategy
- 26 million single-dose Gardasil doses procured via Gavi, the Vaccine Alliance
- Indigenous CERVAVAC to ensure long-term sovereign sustainability
This reflects a dual approach:
- Immediate scale (international procurement)
- Long-term resilience (domestic manufacturing)
2. Digital & Supply Chain Backbone
- U-WIN portal: Beneficiary registration & tracking
- eVIN (Electronic Vaccine Intelligence Network): Real-time cold-chain monitoring
Demonstrates integration of digital governance into immunization systems.
3. Delivery Strategy: Dual-Channel Model
(A) School-Based Delivery
- Classes 5–10 targeted
- High density, low wastage
- Overcomes gender mobility barriers
(B) Community Outreach
- Mobile health teams
- Reaching out-of-school and marginalized girls
This mirrors India’s success in adolescent health campaigns.
IV. Lessons from the Sikkim Model (2018–2019)
Sikkim pioneered statewide HPV vaccination.
Key Outcomes:
- 95% first-dose coverage
- 90% second-dose completion
Best Practices:
- Strong political commitment
- Health–Education department synergy
- Mandatory school enrollment leverage
- Crisis communication against vaccine hesitancy
This model informs the national roadmap.
V. Socio-Economic Barriers & Gender Dimensions
HPV vulnerability is closely linked to socio-economic realities:
- 37% early marriage in high-risk areas
- 62% first pregnancy before age 21
- 35% illiteracy among target population
- Gendered mobility restrictions in rural areas
Thus:
School-based vaccination becomes not optional but structurally necessary.
This campaign is therefore:
- A women’s health reform
- A gender empowerment intervention
- A poverty prevention strategy
VI. Governance & Policy Significance (UPSC Angle)
1. Shift to Preventive Healthcare
From reactive tertiary cancer care to primary immunization.
2. Health System Strengthening
- Cold chain expansion
- AEFI surveillance systems
- Digital health infrastructure
3. Intersectoral Convergence
- Health Ministry
- Education Department
- Women & Child Development
- Panchayati Raj institutions
4. Alignment with SDGs
Supports:
- SDG 3 (Good Health)
- SDG 5 (Gender Equality)
- SDG 1 (Poverty Reduction)
VII. Implementation Challenges
1. Vaccine Hesitancy
- Fertility myths
- Religious misinformation
Solution:
- Proactive risk communication
- Community radio & mass media
- Engaging male decision-makers
2. AEFI (Adverse Events) Surveillance
- Transparent reporting essential to maintain trust
3. Screening Integration Gap
Vaccination alone insufficient.
Needs:
- Expansion of HPV DNA testing
- Screening at Ayushman Bharat Health & Wellness Centres
- Referral linkages
4. Financial Protection Gaps
Even free treatment incurs:
- Travel costs
- Caregiver costs
- Income loss
Recommendation:
- Patient Navigation Programs
- Logistical support for cancer care
VIII. Strategic Roadmap Toward 2030
To achieve elimination:
- Integrate HPV vaccination into routine UIP permanently
- Accelerate screening coverage to meet 70% target
- Scale indigenous CERVAVAC production
- Strengthen patient navigation systems
- Institutionalize communication strategy against misinformation
India must shift from “campaign mode” to systemic resilience mode.
IX. Critical Evaluation (Balanced View for Mains)
Strengths
✔ Evidence-based single-dose strategy
✔ Strong digital backbone
✔ School-based model reduces inequity
✔ Domestic vaccine manufacturing capability
Concerns
⚠ Sustainability post-Gavi support
⚠ Rural hesitancy
⚠ Screening infrastructure gaps
⚠ Monitoring & evaluation consistency
Conclusion
India’s 2026 HPV Vaccination Drive marks a decisive shift in women’s public health governance. By prioritizing primary prevention, leveraging digital infrastructure, and integrating socio-economic realities into implementation design, the programme has the potential to transform cervical cancer from a leading killer into a preventable disease.
If sustained and integrated into routine immunization, this initiative could become one of India’s most consequential public health achievements — advancing the vision of a “Cancer Mukt Bharat” and aligning with global elimination targets.
UPSC Enrichment Section
Syllabus Reference:
GS Paper II – Government policies and interventions for development in health and social sector.
Sample 15-Marker Question:
“Discuss the significance of India’s nationwide HPV vaccination drive in achieving cervical cancer elimination. What implementation challenges must be addressed?”